How many real Covid-19 cases are there?
By Generali Investments’ Research Team
Estimating the real total infected is key because the spread of the virus obviously depends on true, not on official cases. Reported cases are probably a fraction of the actual total. What is worse, the share is believed to vary wildly across countries, from those who tested extensively and even randomly (Korea) to those where only the seriously ill get tested (Italy, up to a point). Random testing is the only way to gauge the actual share of the population that has been infected. Unfortunately, the tested population is almost invariably heavily selected.The most dependable measure are in all likelihood the fatality counts, although these are known to have been underestimated as the situation of the health system worsened.
Fatalities are the tip of the iceberg. Observed deaths - perhaps the most precise of available measures - can be used for assessing the number of current true cases, reported and unreported, given a number of parameters. Some of these depend on the nature of the disease (time to death, incubation etc.) others depend on the country, i.e. on the density of social groups, the health system, fatality rate, doubling time, etc. To move from deaths to (current) true cases in one given day take the current mortality rate, suppose 1%. This means 1 death today indicates 100 infected at the time of infection. Now we need to calculate the evolution from 100 infected back then when the dead person got infected until today. From the time to death τ (estimated at 17.3) and then the doubling time (the time it takes for cases to double) estimated at 6.2 we can estimate the number of true cases today. This procedure has the benefit of estimating the current true cases, including asymptomatic spreaders.
The fatality rates of Covid-19 reported across the world have been the most diverse, peaking at over 13% in Italy, while the general consensus between epidemiologists is that it be one order of magnitude lower (nearly one tenth of the observed rates), even adjusting for the age structure of the population and for other risk factors like pollution and concurrence of other lung diseases. Even over homogeneous populations, obtaining a consistent estimate of mortality (deaths over the entire population) and fatality (deaths over the infected population) rates obviously depends on the sample: notoriously, during the Italian outbreak the vast majority of the people who got tested were seriously ill, to the point of showing strong symptoms or even of needing intensive care. Ideally, one would want to do a random trial on, respectively, the entire population or a randomly chosen population of infected, without the milder cases going unnoticed.
The Diamond Princess case. What is perhaps the closest to an experiment of this kind happened when the Covid-19 spread on the cruise ship Diamond Princess (see here). The ship contained 3,711 passengers and crew, of which 700 got infected. While the infection rate got magnified by the close confinement conditions, the sample of infected people was reasonably close to randomness (despite some prevalence of older people) and, especially, everybody on board was tested. There were 7 dead in the cruise ship (1% of cases), a number too low for dependable estimation. That said, when researchers used the methodology, i.e. the share of people with mild symptoms, or even asymptomatic (18%), to estimate the true number of infected in the Wuhan outbreak, they come up with a similar “true” fatality rate of 1.1%, against the official estimate of 3.8%.
Underreporting While in “normal” conditions, for the reasons given above, one can expect “most” of Covid-related deaths to be reported, experience taught us that there will always be some degree of underestimation. This effect will typically be non-linear, as unreported Covid-19 deaths will begin to occur massively during the peak of the emergency, as (if) the health system is overwhelmed and resources are not enough to test all the dead for Covid antibodies: especially those who do not even get to the hospital and die at home. The most popular way to assess the actual Covid-related mortality has been to compare reported Covid-19 deaths to the increase observed over the “normal” (average) mortality of the relevant region. According to this method, for example, in the Italian province of Bergamo the statistical “extra mortality” has been more than double the reported number of official Covid-19 deaths. According to recent coverage by FT, the size of the underreporting might well be as high as 60%.
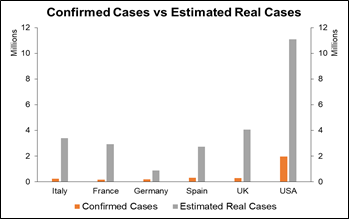
So, how many actual cases have there been? Based on this line of reasoning, one could estimate the order of magnitude of the total infected in different countries taking the total number of dead, perhaps allowing for an underreporting rate of between 10 and 60%; assuming a case fatality rate of about 1.5% in the Western world -- where the share of the elderly and of the people affected by other risk-enhancing pathologies (obesity, diabetes, asthma) is higher – and 0.5 to 1% in emerging countries and developed South-East Asia. From this gauge the true number of infected, symptomatic and asymptomatic, gross of the recovered, as being around 100 times the dead in the West, and between 150 and 200 times in Africa and SEE. In any case, we can estimate the actual infected, current and past, to be two orders of magnitude higher than the dead: which would take the count, for Italy, to about 3 million; or, for the USA only, to the impressive figure of around 11 million people who are, or have been, carrying the virus. Too many to be safe, too few to grant any kind of herd immunity.